Posts Tagged ‘GW Pharmaceuticals’
CLEAR’s Submission To The Parliamentary Inquiry Into Medicinal Cannabis
This was the response that CLEAR submitted to the APPG in February 2016. In March 2016, Roland Gyallay-Pap, then managing director of CLEAR and Peter Reynolds, president, were called to give oral evidence to the Inquiry.
A PDF copy of this document may be downloaded here.
Introduction
In June 2015 the All-Party Parliamentary Group for Drug Policy Reform (APPG) published a short report arguing for a rescheduling of cannabis to make it more widely available for medical use. Following the publication of that report there are a number of key questions remaining that it would like to address by means of a Short Inquiry.
CLEAR Cannabis Law Reform has been asked to submit evidence to the Inquiry in answer to these specific questions:
- Whether switching the medical status of cannabis from schedule 1 to a less restrictive schedule would be beneficial?
- What do you understand to be the range and extent of unofficial use of cannabis for medical purposes?
- What has been the impact of the current schedule 1 status on research into the medicinal uses of cannabis?
- Is there useful evidence emerging from the regulation of cannabis in over 20 US states and elsewhere and what does it tell us about the case for cannabis to be included in the UK pharmacopeia?
- What would be the implications of licencing cannabis for medicinal use following a change in Schedule?
- What role could EU regulations play in developing the potential for the medicinal use of cannabis?
We have also added a further response with additional information.
- Access to prescribed Bedrocan medicinal cannabis is already possible based on careful use of loopholes and errors in existing English law.
Whether switching the medical status of cannabis from schedule 1 to a less restrictive schedule would be beneficial?
Yes, we consider that switching cannabis from schedule 1 to a less restrictive schedule would be beneficial, both so that it could be prescribed by doctors as medicine and so that it could more easily be used in research into its use and effects.
Cannabis has been in schedule 1 of the Misuse of Drugs Regulations1 (MoDR) since the Misuse of Drugs Act 19712 (MoDA) came into force. Drugs in schedule 1 are specified as having no medicinal value. However, an inquiry by the House of Lords Science and Technology Committee published in 19983 recommended that doctors should be permitted to prescribe cannabis and that it should be moved to schedule 2. Strangely the government’s response to this recommendation was further to tighten restrictions by the Misuse of Drugs (Designation) Order 20014, which designates cannabis under section 7(4) of MoDA so that it is unlawful “for a doctor, dentist, veterinary practitioner or veterinary surgeon, acting in his capacity as such, to prescribe, administer, manufacture, compound or supply” it.
In fact, cannabis has already been re-scheduled into schedule 4 under the international non-proprietary name of nabiximols (Sativex)5. Although this is specified as being an extract of THC and CBD, it is clear from statements by the manufacturing company, GW Pharmaceuticals, that nabiximols is whole plant cannabis. Dr Geoffrey Guy, founder and chairman of GW, is on the record:
“Most people in our industry said it was impossible to turn cannabis into a prescription medicine. We had to rewrite the rule book. We have the first approval of a plant extract drug in modern history. It has 420 molecules, whereas every other drug has just one.”6
GW pharmaceuticals has confirmed that this quotation is accurate.7
The MHRA has chosen to issue a marketing authorisation8 for nabiximols (Sativex) by regarding it as only a two molecule medicine. The marketing authorisation is therefore at best inaccurate, at worst dishonest.
What do you understand to be the range and extent of unofficial use of cannabis for medical purposes?
In 2011, CLEAR commissioned independent, expert research from the Independent Drug Monitoring Unit (IDMU). The report, ‘Taxing the UK Cannabis Market’9, reveals there are three million people using cannabis in the UK regularly (at least once per month). Since then CLEAR has regularly polled its members and followers and consistently one in three of respondents claim at least some part of their use is for medicinal reasons. It is reasonable to estimate therefore that there are up to one million people using cannabis for medicinal purposes in the UK. It is certain that there are hundreds of thousands of medicinal users and previous estimates in the region of 30,000 are far too low.
The most common indications for medicinal use declared by our respondents are chronic pain, fibromyalgia, Crohn’s disease, multiple sclerosis and cancer.
Our interpretation of the responses we have received is that generally cannabis is used as a palliative agent. Some people find it so effective that they consider it to be a ‘cure’ as long as they keep using it. Others find it extremely helpful in reducing the amount of toxic and/or dangerous pharmaceutical medicines they are prescribed. Often the side effects of pharmaceutical medicines are severe and debilitating and cannabis offers a way of minimising these.
CLEAR maintains a Medicinal Users Panel10 which members join in order to gain support in lobbying their MPs and/or attempting to obtain prescribed Bedrocan medicinal cannabis. The active membership of the panel varies between 20 to 80 people. Panel members have also been involved in delegations to meet government ministers and other parliamentarians
What has been the impact of the current schedule 1 status on research into the medicinal uses of cannabis?
In the UK there is very little research into the medicinal uses of cannabis, except that undertaken by GW Pharmaceuticals11. There has been some research carried out into single cannabinoids but the evidence is that the therapeutic effects of cannabis depend on the whole plant ‘entourage effect’.
The allopathic, reductionist approach to medicine, which is reflected in the way that the MHRA regulates medicines, is the fundamental, establishment doctrine that impedes research into cannabis.
Sadly, one of the biggest trials of MS patients, the CUPID study at the University of Plymouth12, intended to look at the many anecdotal reports of benefit, used synthetic THC and consequently the results were disappointing and irrelevant to the claims it sought to test.
It is far easier to obtain funding for research into the harms of cannabis which is undertaken with an almost absurd degree of repetition, most notably by the Institute of Psychiatry at King’s College London (IOPPN).13 It is also worth noting that IOPPN regularly and consistently overstates the results of its research, encouraging the media to report causal effects between cannabis use and mental illness which its research does not support.14
There is a huge stigma around cannabis, largely due to inaccurate, misleading and hysterical press coverage. For instance, neither of the pre-eminent MS patient groups, the MS Society and the MS Trust, will take a stand in support of patients, despite the fact that many use cannabis. Similarly, despite extraordinary human clinical trial results on Crohn’s disease, none of the Crohn’s patient groups will engage with the campaign. Mention cannabis and calls are not returned, people are scared by the stigma. The immediate reaction from all such patient groups is to overlook evidence of benefit and refer to risks to mental health which, in fact, are very low compared to pharmaceutical products. The press, unchallenged by politicians in its disproportionate attention to these risks, bears a heavy responsibility for this stigma and the lack of research.
Unlike many within the reform movement, CLEAR recognises and values the expertise and achievements of GW Pharmaceuticals. However, any doctor or scientist that expresses any interest in medicinal cannabis in the UK is immediately retained or contracted by GW. We receive hundreds of reports of doctors, GPs and consultants, who tacitly and sometimes explicitly support their patients’ use of cannabis but it is impossible to find any doctor who is prepared to speak out publicly. In the few instances where doctors have spoken out on behalf of patients, they have been contacted by Home Office officials and warned. One GP reported that he felt “intimidated”. By contrast, there are tens of thousands of doctors across Europe, Israel and North America who advocate for the use of medicinal cannabis and further research into its applications.
The security and record-keeping requirements for cannabis as a schedule 1 drug15 are wildly disproportionate to the real potential for harm, requiring a high security safe for storage and an audit trail fit for Fort Knox.
In addition the fee for a high THC licence is currently £4700.00 per annum and applications can take more than a year to process. These requirements, delays and corresponding costs severely impede research into medicinal cannabis.
Recently, in response to two government e-petitions, the Home Office issued the following statement:
“In 2013 the Home Office undertook a scoping exercise targeted at a cross-section of the scientific community, including the main research bodies, in response to concerns from a limited number of research professionals that Schedule 1 status was generally impeding research into new drugs.
Our analysis of the responses confirmed a high level of interest, both generally and at institution level, in Schedule 1 research. However, the responses did not support the view that Schedule 1 controlled drug status impedes research in this area. While the responses confirmed Home Office licensing costs and requirements form part of a number of issues which influence decisions to undertake research in this area, ethics approval was identified as the key consideration, while the next most important consideration was the availability of funding.”
We consider this response to be disingenuous and misleading. Cannabis is a special case. It is a combination of hundreds of molecules, unlike other schedule 1 drugs, most of which are single molecules. Also, as is well established in written and archaeological evidence, cannabis has been used effectively for at least 5,000 years as medicine without any evidence of harm.
Furthermore. ethical approval and funding are difficult largely due to the evidence-free scaremongering about cannabis and the consequential stigma, in which the Home Office plays a leading role. Ethical approval and funding do not seem to be a problem in researching potential harms of cannabis. Indeed, as noted above, there is a massive amount of such research even though much of it is repetitive and inconclusive.
Until it is recognised that for many years, under successive governments, the Home Office has been systematically misleading and scaremongering about cannabis, it is difficult to see how an evidence-based decision can be reached. The Home Office regularly makes assertions about cannabis that are completely without evidential support. There is an established prejudice and determination to misinform and this must be tackled at root as it amounts to misconduct and corruption.
Is there useful evidence emerging from the regulation of cannabis in over 20 US states and elsewhere and what does it tell us about the case for cannabis to be included in the UK pharmacopeia?
There is a vast amount of peer-reviewed, published evidence of the safety and efficacy of cannabis as medicine. Much of this arises from research carried out in the USA, the Netherlands and Israel, where medicinal cannabis regulation has been in place for many years.
It is a populist myth, promoted by the Home Office, the press, the BBC and the prohibitionist lobby, that there is no evidence supporting the use of cannabis as medicine.
In February 2015, a delegation of medicinal cannabis users from CLEAR met with George Freeman MP, the life sciences minister, at the Department of Health who is largely responsible for medicines regulation. At the conclusion of the meeting, Mr Freeman requested CLEAR to produce a summary of the available evidence.
The result is the paper ‘Medicinal Cannabis:The Evidence’16 (MCTE) which has received international acclaim, so much so that in association with Centro de Investigaciones del Cannabis (CIC), a Colombian non profit association, a Spanish language version has been published.
MCTE was submitted to George Freeman MP in April 2015. Since then he has repeatedly refused to meet CLEAR again or respond to us directly, even after multiple requests from individual MPs representing CLEAR members. His only responses, received through third parties, fail to address the evidence at all. He simply refers to the legal status of cannabis, the theoretical availability of Sativex and the MHRA process for issuing marketing authorisations in respect of medicines.
This refusal to engage, acknowledge or properly consider the very large amount of evidence that is available is indicative of an inexplicable prejudice within government. Although conspiracy theories abound, it is difficult to understand why ministers adopt this position.
Cannabis was one of the most used medicines in the British pharmacopeia until only about 100 years ago. It could be restored immediately by a stroke of the Home Secretary’s pen to remove it from schedule 1. This would immediately make it possible for doctors to prescribe medicinal cannabis from Bedrocan17, the Netherlands government’s exclusive contractor.
Bedrocan cannabis is carefully regulated by the Netherlands government’s Office of Medicinal Cannabis. It is available in five different THC:CBD ratios. It is already exported to many countries in Europe and the company has established itself in Canada as well. It is less than a tenth the cost of Sativex for equivalent cannabinoid content and can be consumed either by a medical vapouriser or as an infusion.
No minister in this or any previous government has ever presented a coherent reason for the refusal to allow cannabis to be used as a medicine. Their only response is to fall back on largely spurious or exaggerated claims about the harms of recreational use.
What would be the implications of licencing cannabis for medicinal use following a change in Schedule?
Cannabis would not need to be ‘licenced’ for medicinal use following a change in schedule. As soon as it removed from schedule 1, doctors would be able to prescribe it and businesses interested to grow, process and develop cannabis medicines would be able to obtain cultivation/possession licences from the Home Office.
Medicines are no longer ‘licenced’ in the UK. The MHRA grants marketing authorisations. The initial fee, simply for filling in the application form is £103,000.00, thus prohibiting any but the very largest, established businesses from even considering such a venture. The very term ‘marketing authorisation’ reveals the mindset of medicines regulators which is now more about commercial interests than the evaluation of the safety and efficacy of medicines.
The MHRA does have a regulatory scheme for ‘Traditional Herbal Registration’ (THR) but it only applies “if the medicine is used for minor health conditions where medical supervision is not required.”. An application for a THR for cannabis could not be made while it remains in schedule 1 but, if granted, would not permit its use for many conditions where there is excellent evidence of its efficacy.
The MHRA is locked in an inflexible, unscientific and restrictive process which can only evaluate medicines which are either one or two molecules. Its process is designed for synthetic, potentially very dangerous molecules and is entirely unsuitable for a plant based medicine such as cannabis. This is why, as explained above, Sativex has been improperly regulated as containing only two molecules: THC and CBD.
When the Sativex (nabiximols) patent expires, independent analysis of the medicine would certainly demonstrate that it is whole plant cannabis oil. Presumably alternative and/or generic versions could then be produced. However, by any standards, for all parties, the regulation and scheduling of Sativex is inaccurate, if not dishonest, and needs revision.
If cannabis is removed from schedule 1, most appropriately to schedule 4 alongside Sativex, in our judgement there will be a large number of businesses applying for cultivation/possession licences for research which will eventually result in applications for marketing authorisations. In the meantime, it can only be described as cruel and evidence-free not to permit doctors to prescribe Bedrocan, a safe, effective medicine already regulated by another European government.
It is likely that enabling the prescription of Bedrocan would result in substantial savings to the NHS medicines budget. However, any idea that this could be quantified based on existing evidence is fanciful. Certainly, compared to existing prescription medicines and Sativex, Bedrocan is very inexpensive, probably less than 10 euros per patient per day. However, the complexity of calculating which medicines it could replace by individual, partly or wholly and for how long makes the exercise so hypothetical as to be meaningless.
It must be true that once local, UK-based cultivation of medicinal cannabis was permitted, prices would reduce even further.
What role could EU regulations play in developing the potential for the medicinal use of cannabis?
Aside from France and Ireland (which is moving rapidly towards drugs policy reform), every other EU country has a more intelligent, compassionate and evidence-based policy towards medicinal cannabis. Based on existing policy and its record, the UK government would simply refuse to comply with any EU regulation of medicinal cannabis.
Under the Schengen Acquis (of which UK is a signatory, though not to the full Schengen Agreement), if a medicine is prescribed to a resident of a member state, that resident may travel to other member states with up to three month’s supply under the protection of a Schengen certificate. The effect of this is that a resident of the Netherlands, Belgium, Finland, Germany, Italy, etc. can bring prescribed cannabis, likely Bedrocan, into the UK and use it without restriction.
The crucial test here is residency, so it is not possible for a UK resident to travel to another country, obtain a prescription and then return to the UK legally with cannabis. Presently, a Schengen certificate for a UK resident has to be issued by the Home Office. Strangely and in contravention of this explicit provision, Norway (Non EU but a signatory to Schengen) does permit its residents to obtain prescriptions, usually in the Netherlands, and return home with cannabis.
It is also likely that given the hostility towards EU regulation, adding cannabis into that debate would be counterproductive. It would be used as another stick with which to beat the EU.
Access to prescribed Bedrocan medicinal cannabis is already possible based on careful use of loopholes and errors in existing English law.
As some members of the APPG are aware, CLEAR has been involved in trying to obtain legal access to prescribed Bedrocan since 2012. We now have approximately a dozen members who regularly receive private prescriptions from their doctors (both consultants and GPs) and travel to the Netherlands to have them dispensed.
In all instances, these individuals have either declared their medicine at customs and/or have made prior arrangements with the Border Force, producing supporting documentation.
This is possible because of errors and inconsistencies in the MoDA and the MoDR. All English drugs legislation, including the recent Psychoactive Substances Act 2016, is badly drafted, contradictory and scientifically illiterate.
The principle active ingredients of cannabis are delta-9-THC and cannabidiol (CBD). Bedrocan products are specified with different ratios of these substances. While cannabis is classified in schedule 1, so is delta-9-THC but it is also in schedule 2 described as dronabinol, which is the international non-proprietary name (INN) for delta-9-THC. CBD is not a controlled drug.
Therefore, if a doctor is prepared to write a prescription e.g. dronabinol (Bedrocan 22%) or dronabinol (Bediol 7.5%), three month’s supply of the medicine may be legitimately imported as a schedule 2 drug.
In the past four years only one CLEAR member has been frustrated in this. He had his medicine seized but he was not prosecuted. An appeal against the seizure failed.
Clearly, the vital factor in this scheme is a doctor who understands the law and the science and is prepared to write the prescription.
References
1. Misuse of Drugs Regulations 2001 http://www.legislation.gov.uk/uksi/2001/3998/contents/made
2. Misuse of Drugs Act 1971 http://www.legislation.gov.uk/ukpga/1971/38/contents
3. House of Lords Science and Technology Committee report 1998 http://www.parliament.the-stationery-office.co.uk/pa/ld199798/ldselect/ldsctech/151/15101.htm
4. Misuse of Drugs (Designation) Order 2001 http://www.legislation.gov.uk/uksi/2001/3997/made
5. Nabiximols (Sativex) https://en.wikipedia.org/wiki/Nabiximols
6. Cambridge News, 24th Jan 2012 http://www.cambridge-news.co.uk/Cannabis-company-enjoys-major-growth/story-22509041-detail/story.html
7. Email corres with Marc Rogerson, GW Pharma, 160312. Attached.
8. Sativex (nabiximols) marketing authorisation, MHRA , 2010 http://www.mhra.gov.uk/home/groups/par/documents/websiteresources/con084961.pdf
9. Taxing the UK Cannabis Market, IDMU, 2011 http://clear-uk.org/media/uploads/2011/09/TaxUKCan.pdf
10. CLEAR Medicinal Users Panel http://clear-uk.org/pages/medicinal-panel/
11. GW Pharmaceuticals website http://www.gwpharm.com/
12. CUPID study, University of Plymouth, 2015 http://www.ncbi.nlm.nih.gov/pubmed/25676540
13. Institute of Psychiatry at King’s College London website http://www.kcl.ac.uk/ioppn/index.aspx
14. King’s College Confirms Institute of Psychiatry Misled Media On Cannabis Brain Study. CLEAR, 2015 http://clear-uk.org/kings-college-confirms-institute-of-psychiatry-misled-media-on-cannabis-brain-study/
15. Controlled Drugs (Supervision of management and use) Regulations 2013, Dept of Health https://www.gov.uk/government/uploads/system/uploads/attachment_data/file/214915/15-02-2013-controlled-drugs-regulation-information.pdf
16. Medicinal Cannabis: the Evidence, CLEAR, 2015 http://clear-uk.org/static/media/PDFs/medicinal_cannabis_the_evidence.pdf Attached
17. Bedrocan BV website http://www.bedrocan.nl/
Home Secretary Invites CLEAR To ‘Enter A Dialogue’ On Cannabis Law Reform.

Rt. Hon. Amber Rudd MP, Secretary of State for the Home Department
In a letter dated 15th August 2016, Amber Rudd, the new Home Secretary, has invited CLEAR to raise “any queries and concerns” about present UK policy on cannabis. This is the first time since 2006, with Charles Clarke, that the UK cannabis campaign has had any direct contact with a serving Home Secretary. It reflects the reality, now recognised in government, that changes in cannabis policy are imminent.
In recent months, there has been a manifest and significant change in attitudes within the Home Office. We have seen this through the process of obtaining a low THC cultivation licence for our partnership with GroGlo Research and Development. The response from the drugs licensing department has been enthusiastic. There has been no difficulty with our declared purpose of producing CBD oil for sale as a food supplement and we are now in detailed discussions on our application for a high THC licence, looking towards clinical trials for a medical product for chronic pain.
As soon as Theresa May announced that Amber Rudd would be heading up the Home Office, I contacted my MP, now Sir Oliver Letwin, thanks to Cameron’s resignation honours list. Although he will not openly support our campaign, in the past year or so he has been very helpful indeed, meeting with me on roughly a monthly basis and helping me navigate through the Conservative government. He has now put me in direct contact with Ms Rudd and I will be preparing a written submission as a preliminary to a face-to-face meeting.
In accordance with CLEAR policy, our first concern is how we can enable UK residents to gain access to medicinal cannabis on a doctor’s prescription. In practice that means Bedrocan products as there is presently no other source of prescribable, consistent, high-quality, herbal cannabis. I would expect that to change very soon though. Both Canada and Israel look like potential near-future sources. GW Pharmaceuticals is undoubtedly considering entering the market and our venture with GroGlo could shift gear depending on how quickly UK policy changes.
We will also be addressing the need for wider reform and a legally regulated market for adult consumers. Although medicinal access remains the top priority, there is no doubt that more overall harm is caused by prohibition of the recreational market. It is this that creates the £6 billon per annum criminal market which is the cause of all the social harms around cannabis. This will need to be handled much more carefully as, due to nearly a century of misinformation and media scaremongering, many people still retain great fear as to what legal cannabis will mean.
The one thing that has been very lacking in the cannabis campaign is pragmatism. Most campaigners for recreational use continue to be lost in a swirl of ‘free the weed’, teenage angst, outrage, revolution and delight in being a rebellious outlaw. That was until 2011 when CLEAR introduced a new approach which has led to more engagement with government than ever before. The emergence of the United Patients Alliance and now the End Our Pain campaign has helped this but these campaigns are focused only on medicinal use
The fact is that we need to work with Theresa May’s government and the anti-Tory tribalism that many still adopt is nothing but an obstacle to reform.
In addressing Ms Rudd, our overall strategy for wider reform will be:
1. A final separation from the ridiculous ‘free the weed’ movement and ‘stoner’ groups which are incapable of understanding how they are seen and despised by wider society.
2. Differentiation between medicinal use and the more controversial legalisation for adult, recreational use.
3. Shift public attention onto scientific and medical evidence rather than the very poor standard of media reporting.
4. End the fake policy that says ‘cannabis is dangerous therefore it must be regulated’. Educate that nearly all the harms around cannabis are caused by its prohibition, not by cannabis itself.
5. Emphasise the importance of harm reduction information, education about excessive use and essential investment in treatment for those who do suffer health harms.
6. Clarify that decriminalisation is no solution and is a dangerous option that would probably increase harm. The product needs to be sold within a properly regulated environment, careful that over-regulation would support a continuing criminal market.
CLEAR and GroGlo Establish First UK Clinical Trials on Cannabis for Chronic Pain.

CLEAR has formed a partnership with the research arm of GroGlo, a UK-based manufacturer of high power, LED, horticultural grow lighting.
The plan is to grow cannabis under a Home Office licence for the production of cannabis oil, both as a dietary supplement and for the development of medical products. To begin with, a low-THC crop of industrial hemp will be planted. We will be using the finola strain, originally developed in Finland and known for its short stature and early flowering. Unlike hemp grown for fibre, finola is usually grown for seed and only reaches a height of 160 – 180 cm but we will be removing male plants before they produce pollen and cultivating the female plants to produce the maximum yield of oil from their flowering tops.

Finola Industrial Hemp
The low-THC oil will be marketed as a dietary supplement, commonly known as CBD oil. There is already a burgeoning market in the UK for CBD products, all of which is currently imported from Europe or the USA. In the USA, the CBD products market was said to be worth $85 million in 2015 so there is huge potential here at home. Aside from the benefit of being UK grown and processed, we anticipate achieving a CBD concentration of about 40%, which is higher than most products already on the market.
Cultivation will be in glasshouses supplemented with LED lighting. GroGlo already has an established glasshouse facility in the east of England. Initial trials will experiment with adjusting the LED technology to provide a changing blend of light wavelengths at different stages of plant growth. This is GroGlo’s area of expertise -combining LED lighting and plant sciences, including existing relationships with some of Europe’s top universities. Professor Mick Fuller, GroGlo’s director of plant science, will lead this research and development process.

Professor Mick Fuller
During the R&D phase, CO2 extraction of oil will be carried out under laboratory conditions at universities in York and Nottingham which already have extensive experience of the process. Each crop will be measured for yield, cannabinoid and terpene content using high pressure liquid chromatography (HPLC). Safety testing will also look for the presence of heavy metals and other contaminants. The results of testing will be fed back into cultivation and extraction processes to maximise yield and quality.
It is anticipated that the first batches of low-THC oil will be ready for market in six months. We are already in discussions with potential distributors and wholesalers. The CBD market in the UK is ripe for an effective marketing campaign which could build a very substantial business for whoever gets it right.
Once we are successfully achieving our production goals with low-THC cannabis, the same testing and development process will begin with high-THC varieties of cannabis. The aim will be to produce a range of oils extracted from single strains, selectively bred and stabilised for different THC:CBD ratios.
Professor Fuller says that GroGlo lighting products “are in use worldwide to grow a range of crops, but some 60% of sales currently come from overseas users growing cannabis for legitimate medical use.” He explains that there is an emerging market for all sorts of nutritional and medicinal plant products but cannabis shows particular promise. GW Pharmaceuticals is the only UK company to enter this market and it has become a world leader, despite the current restrictive legislation. He says: “Together with CLEAR we believe we can help bring a range of safe, high quality UK-produced cannabis products to market within a matter of two to three years.”
A key issue in the development of a successful medicinal cannabis product is the method of delivery. Smoking is not an acceptable solution as inhaling the products of combustion is an unhealthy practice but one of the great benefits of cannabis smoked as medicine is very accurate self-titration. That is the effects of inhaled cannabis are felt almost instantly and so the patient knows when they have taken enough or when they need more to achieve the required analgesic effect.
The oral mucosal spray developed for Sativex is unpopular with patients, many complain of mouth sores from its use and it was developed at least as much with the objective of deterring ‘recreational’ use of the product as with delivering the medicine effectively. It strangles the therapeutic benefits of the cannabis oil of which Sativex is composed in order to comply with the concerns of the medicines regulators about ‘diversion’ of the product into what they would term ‘misuse’. Absorption of the oil is quicker through the mucous membranes of the inside of the mouth than through the gastrointestinal system but, inevitably, some of the oil is swallowed and the pharmacology of cannabis when processed through the gut and the liver is very different.
We believe the best option is a vapouriser device and our intention is to source a ‘vape pen’ of sufficient quality to operate within clinical standards of consistency and safety. Vapourising cannabis oil avoids inhaling the products of combustion but still enables accurate self-titration of dose. A vape pen would provide a handy, convenient and very effective method of consuming medicinal cannabis. However, aside from the technology itself, initial research shows that vapour is more effectively produced when the oil is blended with either vegetable glycerin (VG) or propylene glycol (PG). Establishing the correct ratio of VG or PG to the oil is another important task.
We anticipate that clinical trials for the use of cannabis oil in treating chronic pain could start within two years. We want to compare different oils, ranging from high-CBD to equal ratios of THC:CBD and high-THC content. Prior to that we have to overcome the challenges of cultivation, oil extraction, vapouriser development and assemble the necessary research team and gain ethical approval for the trials. Recruitment for the trials will start in about 18 months time. If you wish to be considered please email ‘paintrials@clear-uk.org’ with brief details of your condition (no more than 100 words). Do not expect to hear anything for at least 12 months but your details will be passed to the research team as a potential candidate.

Mike Harlington, Managing Director of GroGlo
CLEAR is promoting this venture simply because someone needs to do something to make this happen. For all the campaigning and lobbying of MPs and ministers, at the end of the day, the plants have to be grown and the various legislative hoops have to be jumped through. We cannot wait any longer for a radical change in the law. We have to progress through the government’s regulatory regime if we want to bring real therapeutic benfit to patients.
This opportunity arises because of the vision of GroGlo’s managing director, Mike Harlington and the team of experts he has built around him. There is huge demand for legitimate medicinal cannabis products in the UK which is only going to increase with the inevitable progress towards law reform and increasing awareness of the benefits of cannabis. Together, CLEAR and GroGlo are bringing the great hope that medicinal cannabis offers closer to reality than ever before.
GW Founder And Chairman, Geoffrey Guy, Explains Sativex.
“Most people in our industry said it was impossible to turn cannabis into a prescription medicine. We had to rewrite the rule book. We have the first approval of a plant extract drug in modern history. It has 420 molecules, whereas every other drug has just one.”

This Is The Future Of Cannabis. For Medicine, Nutrition And Pleasure.

One of these vape pens contains Blue Dream sativa cannabis oil, 91% THC, the other is Hindu Kush indica cannabis oil, 85% THC and the spare cartridge has the dregs of some New York City Diesel sativa, 85% THC. You can’t tell which is which to look at them but each has a distinctive flavour and effect. They’re not completely odour free but almost.
This is the future of cannabis as a consumer product. It is cleaner, neater, handier, healthier and better for you than raw herbal cannabis. Most importantly, for medicinal applications, it homogenises all the compounds into an oil of consistent quality and content meaning that dosage and effect at last becomes predictable and reliable.
High CBD Oil For Medical Use
I have been investigating this theory for some time but my recent trip to Colorado enabled me to conduct some practical experiments and more thoroughly understand how this idea can work. I am now convinced that this is the way forward for the cannabis industry. Once we achieve legalisation in the UK, which is inevitable, probably in about five years, these pens are how cannabis will become available as a consumer product on the high street. They are also how medicinal cannabis will be dispensed. Your doctor’s prescription will be fulfilled by a cartridge with the appropriate blend of cannabinoids which you screw onto your battery and use immediately. Batteries will also be supplied on prescription, in the same way that syringes or blood glucose meters are for diabetics.
In Colorado dispensaries these pens are already available in a choice of strains and blends. Currently, the popular products contain 250 mg of THC in a blend of cannabis oil and propylene glycol (PG), just as e-cigs contain a nicotine oil and PG.
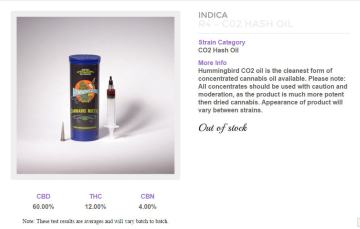
Alternatively, you can buy the oil of your choice and fill the cartridges yourself. This is undoubtedly the way to do it and a wide choice of oils is available, made by CO2 and solvent extraction processes. The Farm, my favourite dispensary in Boulder, is already supplying cannabinoid blends such as a 60% CBD, 12% THC, 4% CBN product which is clearly for medicinal use. I have no doubt that soon we will see a Charlotte’s Web product and Sativex-like blends with equal ratios of THC:CBD. Other, more sophisticated blends of other cannabinoids and probably terpenes will soon follow.
However, I am certain that some propylene glycol is a good thing. The oil vapes much better when diluted and PG is nothing to worry about, it is in many health, cosmetic and food products. It has many uses. It’s a solvent, humectant (keeps things moist), preservative and it helps absorption of some products. It is non-toxic.
There is further development work to be done. I believe there is a ‘sweet spot’ for the correct amount of PG, probably around 20%. I also think the battery and cartridges can be improved, particularly for medical use. Once this is achieved, a product like this with perhaps a 60:40 THC:CBD ratio should form the basis of an application to the Medicines and Health products Regulatory Agency (MHRA) for a marketing authorisation. It will knock Sativex into a cocked hat. In fact, if GW Pharma aren’t investigating this already then they are failing in their duty to shareholders. I shall certainly be doing all I can to research and facilitate the funding to bring such a product to market.
Yes, this is the future of cannabis. Imagine the packaging, marketing and merchandising opportunities for the recreational market. Understand the overwhelming benefits of this as medicine against the raw, herbal product. Yes, I know some will object and the tired old hippy luddites will say it’s a sell out and many more Big Pharma conspiracy theories will emerge but this is the future. Remember you heard it here first.
The Man Who Smashed UK Cannabis Prohibition – And Looks Set To Do The Same In America.

Dr Geoffrey Guy
Across social media, it’s ‘on message’ to despise Big Pharma and to promote the idea that government and pharmaceutical companies are engaged in the business of making people ill and feeding them with drugs in the pursuit of profit.
In the cannabis campaign, it’s virtually compulsory to abuse, defame and promote conspiracy theories about GW Pharmaceuticals, the world’s leading developer of cannabis-based medicines.
Now GW Pharma is hardly ‘Big Pharma’. It’s annual revenues for 2014 were £30 million. By contrast, Pfizer’s 2014 revenue was $50 billion. But such trifling facts are of no concern to the keyboard warriors and trolls that plague the cannabis campaign and bring it into disrepute every day.
In any case, I’m not sure whose message this is and why anyone buys into this hate-filled invective and unjust condemnation of an industry that has saved so many lives. Antibiotics, vaccines and, yes, chemotherapy products have saved or extended millions of lives. The most profitable pharmaceutical product of all time, Zantac (ranitidine), cures or prevents stomach ulcers and has prevented millions from having to undergo major surgery. Certainly, as in any industry, there have been mistakes, things have gone wrong and much could be improved but overall, the pharmaceutical industry is a huge force for good in our world.
Those engaged in these bitter, vindictive, online campaigns are largely sheep, ignorant of the facts and simply jumping on another hysterical bandwagon that they understand nothing about. They complain about the pursuit of profit and that money is being made from medicines and healthcare. It’s a strangely socialist and anti-business attitude, particularly as so much of it comes from America, supposedly the home of free enterprise where the maverick and outsider who triumphs against all the odds is usually revered.
Dr Geoffrey Guy, who founded GW Pharmaceuticals in 1998, is such a man. He has broken the UK government’s prohibition of cannabis by outwitting a regulatory process run by the Home Office and the Medicines and Healthcare Products Regulatory Agency (MHRA) that is corrupt, dishonest and denies scientific evidence. In my view, he deserves great admiration and should be seen as a hero by cannabis campaigners, not as the villain that he is often portrayed.
Now, both GW’s lead products, Sativex and Epidiolex, look set to gain FDA approval in the US. This will be a fantastic achievement for Dr Guy and all his colleagues. It’s also something that we Britons should be immensely proud about. Even though America is a very long way ahead of us in understanding and using cannabis as medicine, it is British science and expertise that is breaking down US federal prohibition. Soon most Americans will have state sanctioned access to medical marijuana but also the option for doctor-prescribed cannabinoid medicine of unparalleled quality and consistency.
Of course, for now GW Pharma stands against the use of raw herbal cannabis and at present that’s a rational business decision but I won’t be at all surprised if in future it moves into that market too. There are already unconfirmed rumours that GW is considering entering the CBD market.
This is a story of enormous courage, innovation and triumph against all the odds. It is in the finest tradition of British ingenuity and business skill. Since the Middle Ages we have led the world in engineering, science and technology. Geoffrey Guy is another world leader from Britain, this small island that has given birth to so many. Surely, at least a knighthood, possibly a Nobel prize must be coming his way soon. Even if the curmudgeonly, loud mouthed critics of today attack him, in future years he will be seen as a great pioneer of medicine and he will deserve his place in history.
Shocking BBC Report On Herbal Products Highlights Problems With Cannabis Regulation.
It seems that unless you choose a herbal product with a THR mark you can have no certainty at all about what you are buying.
An excellent report on the BBC’s ‘Trust Me I’m A Doctor‘, reveals that the industry is rife with confidence tricksters, fraudsters and probably some well-meaning incompetents. How can you know what you’re getting in a herbal product? This has major implications for the medicinal use of cannabis and the businesses that will be needed to supply the product when it is legally available.
The THR mark is Traditional Herbal Registration as regulated by the Medicines and Healthcare products Regulatory Agency (MHRA). It costs between £600 to £8000 to apply but that’s only if you’re claiming “the medicine is used for minor health conditions where medical supervision is not required (eg a cold).” If you want to claim anything more you have to apply for a marketing authorisation when fees are in excess of £100,000, plus the cost of clinical trials or evidence of your claims and your product’s safety.
This is probably the biggest single problem facing the campaign for medicinal cannabis. We are a round peg which doesn’t fit into any of the government’s square holes.
If we argue for cannabis as medicine, we challenge the reductionist, allopathic establishment which says that medicines are single molecules with directly quantifiable, predictable and consistent results. We cannot fit into the government’s square holes without the sort of approach taken by GW Pharmaceuticals at a cost of tens of millions in development.
That is why the campaign has to focus on removing cannabis from schedule 1, so that doctors may prescribe it as they see fit. Some doctors are ready to do so (a few brave individuals already are prescribing) but it will require a huge campaign to educate others as to why and how to prescribe – and it will not be possible to make any medical claims in that campaign!
The model of cannabis as medicine with different strains providing different therapeutic value just doesn’t fit within any concept of medicine in the UK. That’s like a triangular peg in a square hole.
So perhaps there is little point in an unwinnable campaign to legalise such a drug as medicine when its use is already tarnished by years of propaganda and media scaremongering? It may be a hopeless cause and seeking a more general decriminalisation of the plant might be a wiser course.
This is a question that seems to be unique to the UK. Other jurisdictions, such as the US states, have achieved reform through radical democracy which we do not enjoy in Britain. Canadians have used their courts to enforce access to cannabis as a fundamental human right. Other European countries just seem to be more flexible, intelligent and sympathetic to patients.
On the other hand, it does seem that the MHRA’s THR scheme works and you know what you are getting when you buy a herbal medicine. Otherwise charlatans and confidence tricksters would prevail.
These issues concern not only the campaign for medicinal cannabis but for cannabis law reform as a whole. Until we get to grips with them and develop a coherent approach we may find the UK continues to lag behind the rest of the world.
Medicinal Cannabis AdVan Campaign in London.

Artist’s Impression
Join The Campaign For Medicinal Cannabis On A Doctor’s Prescription.
Despite overwhelming evidence, the UK government insists that cannabis has “no medicinal value”. Present policy is deeply cruel and means that at least one million people in Britain are forced to become criminals in order to deal with their pain, suffering or disability.
We must change this dreadful and unjust policy. It’s time to help rather than persecute people who genuinely need cannabis to improve their health. DONATE HERE.
The AdVan Campaign.
CLEAR is the UK’s leading drugs policy reform group with more than 270,000 followers. We will run an AdVan for one week in central London during the busy pre-Christmas period. This will deliver the simple, direct message that you see above and it will be backed by a supporting PR campaign, lobbying of government ministers and MPs as well as further information on the CLEAR website.
Please donate whatever you can. Every pound makes a difference. We need to raise £3500 to run the AdVan for one week. If we raise more we will run it for longer. DONATE HERE.
Please Donate Now!

Our Simple And Reasonable Request To UK Government.
In 1998, GW Pharmaceuticals was granted a licence to grow cannabis and its cannabis oil medicine, Sativex, is now approved but doctors are prevented from prescribing it because it is so fantastically expensive.
The Dutch government approves a cannabis medicine called Bedrocan which provides exactly the same as Sativex at a tiny fraction of the price. Sativex costs between £375 – £560 per month. Bedrocan costs £35 – £95 per month.
All we ask is that if a doctor prescribes Bedrocan, the Home Office should issue an import licence. This is a narrow, tightly defined reform that will not encourage illicit use but will provide enormous help to some very poorly people. DONATE HERE.
Further Background.
Every year, thousands of medicinal cannabis users are prosecuted for possessing or growing cannabis. Often it is the only medicine that helps them with chronic pain, fibromyalgia, MS, Crohn’s disease, epilepsy, depression or many of the conditions related to aging. It is also used to mitigate the side effects of chemotherapy and HIV/Aids treatments.
In November 2014, the Liberal Democrat MP Norman Baker resigned as a government minister because of the Conservatives’ refusal even to consider drugs policy reform. In July 2014 he met with members of CLEAR and publicly called for cannabis to be legalised for medicinal use. Other ministers are more concerned with stopping people getting high (which they are going to do anyway) than in helping those with severe medical conditions. DONATE HERE.
Other Ways You Can Help
Join CLEAR at http://clearmembers-uk.org
Visit and ‘like’ our Facebook page http://www.facebook.com/ClearUK
Follow us on Twitter @CLEARUK
The Monstrous, Cruel and Ignorant Health Minister Of Jersey.

Deputy Anne Pryke
“It would be irresponsible to allow the importation of cannabis into Jersey. I could not support a proposition to issue a special licence to an individual for the possession of illegal cannabis in its raw form, where neither the quality nor composition of the product, its safety, dosage or levels of individual use could be effectively monitored and I would urge members to vote firmly against this proposition.”
Deputy Anne Pryke, September 2014
Jersey is in an enviable position regarding medicinal cannabis. As a Crown dependency the island has constitutional rights of self-government and judicial independence. It is within the power of Deputy Pryke, the Minister of Health, to issue a licence for Bedrocan medicinal cannabis to be imported from Holland where it is grown legally for medicinal purposes under the regulation of the Dutch government.
A formal States petition has been delivered and Deputy Montford Tadier (the Jersey equivalent of an MP) has requested that an import licence be issued for his constituent, Evelyn Volante who suffers from ulcerative colitis. See a video about her use of medicinal cannabis here. You see above the disgraceful, monstrous, cruel and ignorant words which Deputy Pryke has spoken in response.
Now these are strong words. Too strong for the people at Politics Jersey, where my description of this politician’s conduct met with wide support but then I was kicked out by the admin team who described it as a “personal attack” and an “insult”.
I repeat my description of Deputy Pryke’s conduct as monstrous and cruel. If we cannot call out politicians for actions they take or words they speak in their official capacity then what sort of democracy do they have in Jersey?
To deny anyone access to a medicine that is proven by science to treat a serious medical condition is monstrous and cruel in any and all circumstances. This is a self-evident truth which renders Deputy Pryke unfit to hold any office in government, particularly that of Minister of Health.
Deputy Pryke’s words are also astonishingly ignorant. It is clear that she has been negligent in her duty properly to consider the evidence relating to cannabis and ulcerative colitis.
Cannabis works for all forms of inflammatory bowel disease because the bowel contains CB1 and CB2 receptors which when modulated by cannabis turn off inflammation. Thus it provides more than simply palliative relief. It actually treats the cause of the conditions. For all intents and purposes it is a cure.
Bedrocan cannabis, as approved and regulated by the Dutch government’s Bureau voor Medicinale Cannabis, is strictly quality controlled and its composition and safety are at least as well proven as any pharmaceutical product. As for levels of individual use, this is the same as with any medicine and is controlled by the amount prescribed.
1. The best evidence of all is Ms Volante’s own experience. She already uses cannabis, illegally, and it works better for her than the highly toxic and debilitating pharmaceutical medicines which are offered by her doctor.
2. There is a vast quantity of anecdotal evidence and personal experience from thousands of people around the world using cannabis effectively to treat ulcerative colitis, Crohn’s disease and other forms of inflammatory bowel disease. Deputy Pryke could spend 15 minutes on Google.
3. Many peer reviewed studies show positive benefits and few adverse side effects from treating ulcerative colitis with cannabis. The following are just a small selection
Esposito G et al. Cannabidiol in inflammatory bowel disease: a brief overview. Phytotherapy Research 2012 July; doi:10.1002/ptr.4781
Lahat A et al. Impact of cannabis treatment on the quality of life, weight and clinical disease activity in inflammatory bowel disease patients: a pilot prospective study. Digestion 2012; 85(1): 1-8
Lal S et al. Cannabis use amongst patients with inflammatory bowel disease. European Journal of Gastroenterology and Hepatology 2011 Oct; 23(10): 891-96
Naftali T et al. Treatment of Crohn’s disease with cannabis: an observational study. Israel Medical Association Journal 2011 Aug; 1(8): 455-58
4. GW Pharmaceuticals is presently conducting phase II clinical trials into cannabis for ulcerative colitis.
5. The Meir Medical Center in Israel is also conducting clinical trials and claims 90% of patients achieve significant clinical benefit with no side effects.
UK’s ‘Cruel and Corrupt’ Medicinal Cannabis Policy Exposed By CNN’s Dr Sanjay Gupta.
This clip is from ‘Sanjay Gupta MD’, CNN’s regular medical affairs programme. It was broadcast on Saturday, 16th November 2013.
An hour-long documentary is to follow, probably in March 2014, when Dr Gupta will expose the terrible cruelty, hypocrisy, dishonesty and corruption which is UK policy on medicinal cannabis. The programme will investigate GW Pharmaceuticals and its cannabis medicines Sativex and Epidiolex. It will also feature Bedrocan and its grow facility in Holland and look in detail at the process CLEAR has developed which has so far enabled five members successfully to import medicinal cannabis to the UK.

CNN Camera Crew, Jamie Watling (aka ‘Clarence Clear’), Peter Reynolds and Dr Sanjay Gupta
Although the UK government claims that cannabis has“no medicinal value”, it has licensed GW Pharmaceuticals to grow massive quantities of the plant which it then processes into its hugely expensive medicines. The license, which was issued for research purposes only, was operated unlawfully between 2003, when Sativex became a commercial product, until March 2013 when the Home Secretary retrospectively legalised it.
Most CCGs refuse to provide Sativex because it is so expensive. A month’s prescription of Sativex costs the NHS £560.00. The equivalent from Bedrocan costs between £35.00 and £105.00 depending on which product is prescribed.
Successive governments have failed to act in the interests of British citizens. Ministers have refused even to consider a change in policy and have ignored or rejected all the efforts of CLEAR and other groups to present evidence and make a case on behalf of those who need cannabis as medicine.
Even though medicinal cannabis was the subject most often mentioned in the written evidence to the recent Home Affairs select committee drugs inquiry, it was ignored. No evidence was heard on the subject and no questions were asked.
Peter Reynolds, president and elected leader of CLEAR, commented:
“UK policy on medicinal cannabis is cruel and corrupt. While ministers refuse even to consider reform despite overwhelming scientific evidence, hundreds of thousands of British people persist in pain, suffering and disability which could be relieved by cannabis. The police are used as armed enforcers of GW Pharmaceuticals’ unlawful monopoly, arresting and even imprisoning sick people who are merely trying to improve their health. I want to thank Dr Gupta for his work. While he has travelled thousands of miles to tell this story, UK government ministers hide in their offices with their fingers in their ears.”

