Posts Tagged ‘MHRA’
This Is The Future Of Cannabis. For Medicine, Nutrition And Pleasure.

One of these vape pens contains Blue Dream sativa cannabis oil, 91% THC, the other is Hindu Kush indica cannabis oil, 85% THC and the spare cartridge has the dregs of some New York City Diesel sativa, 85% THC. You can’t tell which is which to look at them but each has a distinctive flavour and effect. They’re not completely odour free but almost.
This is the future of cannabis as a consumer product. It is cleaner, neater, handier, healthier and better for you than raw herbal cannabis. Most importantly, for medicinal applications, it homogenises all the compounds into an oil of consistent quality and content meaning that dosage and effect at last becomes predictable and reliable.
High CBD Oil For Medical Use
I have been investigating this theory for some time but my recent trip to Colorado enabled me to conduct some practical experiments and more thoroughly understand how this idea can work. I am now convinced that this is the way forward for the cannabis industry. Once we achieve legalisation in the UK, which is inevitable, probably in about five years, these pens are how cannabis will become available as a consumer product on the high street. They are also how medicinal cannabis will be dispensed. Your doctor’s prescription will be fulfilled by a cartridge with the appropriate blend of cannabinoids which you screw onto your battery and use immediately. Batteries will also be supplied on prescription, in the same way that syringes or blood glucose meters are for diabetics.
In Colorado dispensaries these pens are already available in a choice of strains and blends. Currently, the popular products contain 250 mg of THC in a blend of cannabis oil and propylene glycol (PG), just as e-cigs contain a nicotine oil and PG.
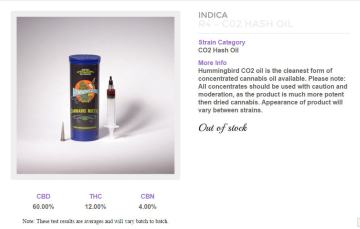
Alternatively, you can buy the oil of your choice and fill the cartridges yourself. This is undoubtedly the way to do it and a wide choice of oils is available, made by CO2 and solvent extraction processes. The Farm, my favourite dispensary in Boulder, is already supplying cannabinoid blends such as a 60% CBD, 12% THC, 4% CBN product which is clearly for medicinal use. I have no doubt that soon we will see a Charlotte’s Web product and Sativex-like blends with equal ratios of THC:CBD. Other, more sophisticated blends of other cannabinoids and probably terpenes will soon follow.
However, I am certain that some propylene glycol is a good thing. The oil vapes much better when diluted and PG is nothing to worry about, it is in many health, cosmetic and food products. It has many uses. It’s a solvent, humectant (keeps things moist), preservative and it helps absorption of some products. It is non-toxic.
There is further development work to be done. I believe there is a ‘sweet spot’ for the correct amount of PG, probably around 20%. I also think the battery and cartridges can be improved, particularly for medical use. Once this is achieved, a product like this with perhaps a 60:40 THC:CBD ratio should form the basis of an application to the Medicines and Health products Regulatory Agency (MHRA) for a marketing authorisation. It will knock Sativex into a cocked hat. In fact, if GW Pharma aren’t investigating this already then they are failing in their duty to shareholders. I shall certainly be doing all I can to research and facilitate the funding to bring such a product to market.
Yes, this is the future of cannabis. Imagine the packaging, marketing and merchandising opportunities for the recreational market. Understand the overwhelming benefits of this as medicine against the raw, herbal product. Yes, I know some will object and the tired old hippy luddites will say it’s a sell out and many more Big Pharma conspiracy theories will emerge but this is the future. Remember you heard it here first.
Another Pack Of Lies On Cannabis From The UK Government.

Yet another cannabis petition amongst hundreds of similar pleas was filed earlier this autumn. This one though is more tightly focused on removing cannabis from schedule 1, which defines it as having no medicinal value. The petition is also commendably concise but characterises itself as a ‘demand‘ that cannabis be rescheduled, an unfortunate choice of words.
 Nevertheless, congratulations are due in that it has exceeded the threshold of 10,000 signatures which means the government must respond. That response is now in and it is predictably dishonest, dismissive and authoritarian in its tone. The Home Office has responsibility for drugs policy so it has drafted the response but it surely must have consulted with the Department of Health.
Nevertheless, congratulations are due in that it has exceeded the threshold of 10,000 signatures which means the government must respond. That response is now in and it is predictably dishonest, dismissive and authoritarian in its tone. The Home Office has responsibility for drugs policy so it has drafted the response but it surely must have consulted with the Department of Health.
In fact, I was told only this week by a senior minister that “… the search into the medicinal use of cannabis is something that falls within the jurisdiction of the Department of Health.” That may be a subtle shift in policy from which we can draw some hope. But I fear that the response to this petition offers no hope at all. It is stubborn, obstinate, inaccurate and in denial of evidence and experience.
To be clear, the Home Office has been systematically lying and misleading the British people about cannabis for at least 50 years. The Department of Health is timid on the issue, leaves the public statements to the Home Office heavies and seems more interested in generating fee income for the Medicines and Healthcare products Regulatory Agency (MHRA), than in actually treating patients effectively.
I analyse the response paragraph by paragraph.
“Herbal cannabis is listed in Schedule 1 as a drug with no recognised medicinal uses outside research. A substantial body of scientific evidence shows it is harmful and can damage human health.”
By far the majority of scientists and doctors now recognise that cannabis has real and significant medicinal uses. Of course it is possible that cannabis can cause harm, as can any substance. However, there is no scientific evidence that shows cannabis as being any more harmful than over-the-counter medicines or many common foods. Professor Les Iversen, chair of the Advisory Council on the Misuse of Drugs, is on the record saying: “cannabis is a safer drug than aspirin and can be used long term without serious side effects”.
“The Government will not encourage the use of a Schedule 1 controlled drug based on anecdotal evidence. It is important that a medicine is very thoroughly trialled to ensure it meets rigorous standards before being licensed and placed on the market so that doctors and patients are sure of its efficacy and safety. “
It is not the government’s role to encourage the use of any drug as medicine, that is the role of a doctor. Only by removing cannabis from schedule 1 can that decision be placed in doctors’ hands. There is a vast quantity of peer-reviewed, published scientific evidence on the medicinal use of cannabis including human clinical trials. It is false to suggest that only anecdotal evidence is available. See ‘Medicinal Cannabis: The Evidence’. Thousands of doctors and millions of patients are sure of the efficacy and safety of cannabis based on existing research, trials and experience. Many commonly prescribed medicines have nowhere near as much evidence behind them as cannabis.
“Cannabis in its raw form (herbal cannabis) is not recognised as having any medicinal purposes in the UK. There is already a clear regime in place to enable medicines (including those containing controlled drugs) to be developed and subsequently prescribed and supplied to patients via healthcare professionals. This regime is administered by the Medicines and Healthcare products Regulatory Agency (MHRA), which issues Marketing Authorisations for drugs that have been tried and tested for their safety and efficacy as medicines in the UK.”
The lack of recognition for the medicinal purposes of cannabis is a grave error with no evidence that supports it. Cannabis is a traditional medicine which recorded history shows has been used safely and effectively for at least 5,000 years. The only thing that stands in the way of cannabis being prescribed by doctors is its schedule 1 status. The MHRA is a diversion and is irrelevant. It exists to trial and regulate new medicines and requires a £100,000 application fee before very costly clinical trials take place. This is an unnecessary obstacle to a traditional medicine which contains more than 400 compounds. The MHRA process is designed for potentially dangerous, single molecule drugs and is not applicable to cannabis.
“It is up to organisations to apply for Marketing Authorisation for products that they believe have potential medicinal purposes so that these can be subject to the same stringent regime and requirements that all medicines in the UK are subjected to.”
Many substances and drugs which have medicinal purposes are regulated either as Traditional Herbal Products or food supplements. It is the schedule 1 status of cannabis which prevents it being regulated and controlled in this way which is far more appropriate given its very low potential for harm and the very wide range of conditions for which it can be useful.
“Since 2010 UK patients can use the cannabis-based medicine ‘Sativex’ for the treatment of spasticity due to multiple sclerosis. ‘Sativex’ can also be prescribed for other conditions at the prescribing doctor’s risk. ‘Sativex’ was rigorously tested for its safety and efficacy before receiving approval, and is distinguished from cannabis in its raw form. It is a spray which is standardised in composition, formulation and dose and developed to provide medicinal benefits without a psychoactive effect. Due to its low psychoactive profile ‘Sativex’ was rescheduled from Schedule 1 and placed in Schedule 4 Part 1 to enable its availability for use in healthcare in the UK.”
Sativex is a massively expensive form of cannabis oil which is not prescribed because of its cost. It is at least 10 times the price of Bedrocan medicinal cannabis as regulated by the Netherlands government which could be immediately made available in the UK. It is a deliberate falsehood to claim that Sativex does not have a psychoactive effect. The statutory document ‘Summary of Product Characteristics’ describes “euphoric mood” as a “common” side effect. The scheduling of Sativex in schedule 4 is a deception requiring 75 words falsely to distinguish it from other forms of cannabis whereas every other drug in every other schedule requires just one word.
“The MHRA is open to considering marketing approval applications for other medicinal cannabis products should a product be developed. As happened in the case of ‘Sativex’, the Home Office will also consider issuing a licence to enable trials of new medicines to take place under the appropriate ethical approvals. “
Cannabis, which contains 400 + compounds is not suitable for MHRA regulation which is designed for single molecule drugs which are potentially dangerous. There is no significant danger from the use of cannabis when prescribed by a doctor. This is already well established in scientific evidence and the referral to the MHRA is a diversion and an excuse for failing simply to put the decision in doctors’ hands.
“In view of the potential harms associated with the use of cannabis in its raw form and the availability of avenues for medicinal development, the Government does not consider it appropriate to make changes to the control status of raw or herbal cannabis. “
The government has offered no evidence of the potential harms to which it gives such weight. No “development” of cannabis is required. It is a traditional medicine consisting of the dried flowers of the cannabis plant.
“The Government’s view is that the Misuse of Drugs Act 1971 and regulations made under the Act continue to facilitate the development of medicines which are made from Schedule 1 controlled drugs. The legislation is aimed at protecting the public from the potential harms of drugs and is not an impediment to research into these drugs or development of medicines.”
The government’s view is intransigent and as demonstrated by this response is ignorant of the available evidence. This response reinforces the government’s clear intention not to consider the evidence and simply to deny it. The evidence shows that the potential harms of cannabis as medicine are trivial and inconsequential. If its schedule 1 status was not an impediment to research, there would already be a great deal more research into cannabis as medicine.
“In 2013 the Home Office undertook a scoping exercise targeted at a cross-section of the scientific community, including the main research bodies, in response to concerns from a limited number of research professionals that Schedule 1 status was generally impeding research into new drugs.
Our analysis of the responses confirmed a high level of interest, both generally and at institution level, in Schedule 1 research. However, the responses did not support the view that Schedule 1 controlled drug status impedes research in this area. While the responses confirmed Home Office licensing costs and requirements form part of a number of issues which influence decisions to undertake research in this area, ethics approval was identified as the key consideration, while the next most important consideration was the availability of funding.”
The Home Office is entirely untrustworthy and dishonest on anything to do with cannabis. Researchers, scientists, doctors and those already using cannabis as medicine simply do not trust anything it says on the subject based on long experience of its calculated dishonesty and misinformation.
The Weak And Ineffectual Response Of Most MPs To The Cannabis Debate.
CLEAR has been mobilising its members as never before to lobby their MPs in advance of the cannabis debate on 12th October.
There are honourable exceptions but most responses have been unhelpful, dismissive and have completely failed to deal with the arguments put forward. Most MPs are indoctrinated with the false reporting churned out by the press, scared stiff of the subject and not prepared to look any deeper.
It is a terrible indictment of these people, each of whom costs us about £250,000 per year in salary and expenses. Most simply do not do their job properly, certainly not in the interests of or representing their constituents, mainly they just pursue their own political ambitions and interests. They cannot be bothered to deal with the cannabis issue.
Usually, from both Tory and Labour MPs, the responses parrot the official Home Office line. Most are too lazy to inform themselves about cannabis and the facts and evidence around current policy which costs the UK around £10 billion per annum. This vast sum comprises a futile waste of law enforcement resources and the loss of a huge amount of tax revenue. It provides funding to organised crime, including human trafficking, and does nothing to prevent any health or social harms around cannabis. In fact, if anything it maximises these harms, endangering health, communities and the whole of our society by enforcing a policy which is based not on evidence but on prejudice. Source: http://clear-uk.org/media/uploads/2011/09/TaxUKCan.pdf
Paul Flynn MP
As Paul Flynn MP, said in the House on 14th September:
“There is [a debate] in a fortnight’s time, on a subject that terrifies MPs. We hide our heads under the pillow to avoid talking about it, but the public are very happy to talk about it in great numbers. That subject is the idea of legalising cannabis so that people here can enjoy the benefits enjoyed in many other countries that do not have a neurotic policy that is self-defeating and actually increases cannabis harm.”
Source: http://www.theyworkforyou.com/whall/?id=2015-09-14a.185.0#g194.0
Below I reproduce a reply from one MP. This is the standard MP line on cannabis. The words may vary slightly but essentially this is the response that the Home Office enforces and, irrespective of party, these are the disingenuous statements that MPs hide behind.
“I believe cannabis is a harmful substance and use can lead to a wide range of physical and psychological conditions. I therefore do not support the decriminalisation or legalisation of cannabis at this time.
I welcome that there has been a significant fall in the numbers of young people using cannabis, and the number of drug-related deaths among under-30s has halved in a decade and I would not want to see this progress undermined.”
Stating cannabis is harmful is meaningless and and an evasion of the question. Anything can be harmful. Such an assertion only has any meaning when in comparison to other substances. In fact, cannabis is relatively benign, even when compared to many foods. It is much less harmful than energy drinks, junk food, all over-the-counter and prescription medicines and, of course, tobacco and alcohol. Compared to these two most popular legal drugs, cannabis is hundreds of times less harmful. Source: http://www.ncbi.nlm.nih.gov/pmc/articles/PMC4311234/

If cannabis can lead to a wide range of physical and psychological conditions, what are they and how likely is cannabis to bring them on compared to other substances? In fact, the Royal College of Psychiatrists, whose publications are often presented as evidence of cannabis harms, states unequivocally
“There is no evidence that cannabis causes specific health hazards.”
Source: http://www.rcpsych.ac.uk/healthadvice/problemsdisorders/cannabis.aspx
There is a reported fall in cannabis use from the British Crime Survey. However, the Association of Chief Police Officers reports ever increasing incidents of cannabis cultivation and there has been a massive surge in the use of ‘legal highs’ or novel psychoactive substances. Without exception, these are far more harmful than cannabis and their very existence is the product of government policy. In places such as Holland and the US states that have legalised, there is no problem at all with such substances.
As for “drug-related deaths”, this is classic disinformation. What does it have to do with cannabis? Are our MPs so badly informed that they cannot distinguish between different drugs? Sadly, in many cases the answer is yes. Even so, this is a false claim. The latest figures show an increase in the number of drug poisoning deaths to the highest level since records began in 1993. So much for the claimed “progress”. Source: http://www.ons.gov.uk/ons/dcp171778_414574.pdf
Just recently MPs have started to address the question of medicinal use, almost certainly because of the rising clamour from people in pain, suffering and disability. Also because the UK is now a very long way out of step with the rest of Europe, the USA, Canada, Israel, Australia and most ‘first world’ countries. Source: http://clear-uk.org/static/media/PDFs/medicinal_cannabis_the_evidence2.pdf
“I am aware that one of the issues raised is around enabling the use of cannabis for medicinal purposes. I know that cannabis does not have marketing authorisation for medical use in the UK, and I understand that the Medicines and Healthcare products Regulatory Agency can grant marketing authorisation to drug compositions recognised as having medicinal properties, such as in the case of Sativex.”
A marketing authorisation from the Medicines and Healthcare products Regulatory Agency (MHRA) is a deliberate diversion from the issue. Medicines do not have to have an MHRA marketing authorisation. Doctors can prescribe any medicine, licensed or unlicensed, as they wish. However, since 1971, medical practitioners have been specifically prohibited from prescribing cannabis on the basis of no evidence at all except minsters’ personal opinions. Source: http://www.legislation.gov.uk/uksi/2001/3997/made.
Applying for an MHRA marketing authorisation costs over £100,000 as an initial fee and clinical trials have to be conducted at a cost of at least the same again. Instead, minsters could simply move cannabis from schedule 1 of the Misuse of Drugs Regulations to schedule 2 alongside heroin and or, more logically, to schedule 4, alongside the cannabis oil medicine Sativex. This would place the whole question of the use of cannabis as medicine in the hands of doctors and not in the politically motivated hands of Westminster. Isn’t that where it should be?
 This is the most important short term objective of the cannabis campaign – move cannabis out of schedule 1. Not only would this enable doctors to prescribe Bedrocan medicnal cannabis as regulated by the Dutch government but it would mean research could start in earnest. The restrictions presently in place on cannabis, because it is schedule 1, make research very expensive, complicated and are a real deterrent.
This is the most important short term objective of the cannabis campaign – move cannabis out of schedule 1. Not only would this enable doctors to prescribe Bedrocan medicnal cannabis as regulated by the Dutch government but it would mean research could start in earnest. The restrictions presently in place on cannabis, because it is schedule 1, make research very expensive, complicated and are a real deterrent.
If you haven’t lobbied your MP on the cannabis debate yet, you still have time to. If you can, get along and see them in a constituency surgery. Full guidance is provided here but you must act now: http://clear-uk.org/guidance-on-how-to-lobby-your-mp-for-the-cannabis-debate/
Most MPs run surgeries on Fridays so that means you have just this coming Friday, 2nd October and the following 9th October.
Please at least ensure you write to your MP. This is our moment and we are having an impact. Make sure you do your bit.
The Man Who Smashed UK Cannabis Prohibition – And Looks Set To Do The Same In America.

Dr Geoffrey Guy
Across social media, it’s ‘on message’ to despise Big Pharma and to promote the idea that government and pharmaceutical companies are engaged in the business of making people ill and feeding them with drugs in the pursuit of profit.
In the cannabis campaign, it’s virtually compulsory to abuse, defame and promote conspiracy theories about GW Pharmaceuticals, the world’s leading developer of cannabis-based medicines.
Now GW Pharma is hardly ‘Big Pharma’. It’s annual revenues for 2014 were £30 million. By contrast, Pfizer’s 2014 revenue was $50 billion. But such trifling facts are of no concern to the keyboard warriors and trolls that plague the cannabis campaign and bring it into disrepute every day.
In any case, I’m not sure whose message this is and why anyone buys into this hate-filled invective and unjust condemnation of an industry that has saved so many lives. Antibiotics, vaccines and, yes, chemotherapy products have saved or extended millions of lives. The most profitable pharmaceutical product of all time, Zantac (ranitidine), cures or prevents stomach ulcers and has prevented millions from having to undergo major surgery. Certainly, as in any industry, there have been mistakes, things have gone wrong and much could be improved but overall, the pharmaceutical industry is a huge force for good in our world.
Those engaged in these bitter, vindictive, online campaigns are largely sheep, ignorant of the facts and simply jumping on another hysterical bandwagon that they understand nothing about. They complain about the pursuit of profit and that money is being made from medicines and healthcare. It’s a strangely socialist and anti-business attitude, particularly as so much of it comes from America, supposedly the home of free enterprise where the maverick and outsider who triumphs against all the odds is usually revered.
Dr Geoffrey Guy, who founded GW Pharmaceuticals in 1998, is such a man. He has broken the UK government’s prohibition of cannabis by outwitting a regulatory process run by the Home Office and the Medicines and Healthcare Products Regulatory Agency (MHRA) that is corrupt, dishonest and denies scientific evidence. In my view, he deserves great admiration and should be seen as a hero by cannabis campaigners, not as the villain that he is often portrayed.
Now, both GW’s lead products, Sativex and Epidiolex, look set to gain FDA approval in the US. This will be a fantastic achievement for Dr Guy and all his colleagues. It’s also something that we Britons should be immensely proud about. Even though America is a very long way ahead of us in understanding and using cannabis as medicine, it is British science and expertise that is breaking down US federal prohibition. Soon most Americans will have state sanctioned access to medical marijuana but also the option for doctor-prescribed cannabinoid medicine of unparalleled quality and consistency.
Of course, for now GW Pharma stands against the use of raw herbal cannabis and at present that’s a rational business decision but I won’t be at all surprised if in future it moves into that market too. There are already unconfirmed rumours that GW is considering entering the CBD market.
This is a story of enormous courage, innovation and triumph against all the odds. It is in the finest tradition of British ingenuity and business skill. Since the Middle Ages we have led the world in engineering, science and technology. Geoffrey Guy is another world leader from Britain, this small island that has given birth to so many. Surely, at least a knighthood, possibly a Nobel prize must be coming his way soon. Even if the curmudgeonly, loud mouthed critics of today attack him, in future years he will be seen as a great pioneer of medicine and he will deserve his place in history.
Shocking BBC Report On Herbal Products Highlights Problems With Cannabis Regulation.
It seems that unless you choose a herbal product with a THR mark you can have no certainty at all about what you are buying.
An excellent report on the BBC’s ‘Trust Me I’m A Doctor‘, reveals that the industry is rife with confidence tricksters, fraudsters and probably some well-meaning incompetents. How can you know what you’re getting in a herbal product? This has major implications for the medicinal use of cannabis and the businesses that will be needed to supply the product when it is legally available.
The THR mark is Traditional Herbal Registration as regulated by the Medicines and Healthcare products Regulatory Agency (MHRA). It costs between £600 to £8000 to apply but that’s only if you’re claiming “the medicine is used for minor health conditions where medical supervision is not required (eg a cold).” If you want to claim anything more you have to apply for a marketing authorisation when fees are in excess of £100,000, plus the cost of clinical trials or evidence of your claims and your product’s safety.
This is probably the biggest single problem facing the campaign for medicinal cannabis. We are a round peg which doesn’t fit into any of the government’s square holes.
If we argue for cannabis as medicine, we challenge the reductionist, allopathic establishment which says that medicines are single molecules with directly quantifiable, predictable and consistent results. We cannot fit into the government’s square holes without the sort of approach taken by GW Pharmaceuticals at a cost of tens of millions in development.
That is why the campaign has to focus on removing cannabis from schedule 1, so that doctors may prescribe it as they see fit. Some doctors are ready to do so (a few brave individuals already are prescribing) but it will require a huge campaign to educate others as to why and how to prescribe – and it will not be possible to make any medical claims in that campaign!
The model of cannabis as medicine with different strains providing different therapeutic value just doesn’t fit within any concept of medicine in the UK. That’s like a triangular peg in a square hole.
So perhaps there is little point in an unwinnable campaign to legalise such a drug as medicine when its use is already tarnished by years of propaganda and media scaremongering? It may be a hopeless cause and seeking a more general decriminalisation of the plant might be a wiser course.
This is a question that seems to be unique to the UK. Other jurisdictions, such as the US states, have achieved reform through radical democracy which we do not enjoy in Britain. Canadians have used their courts to enforce access to cannabis as a fundamental human right. Other European countries just seem to be more flexible, intelligent and sympathetic to patients.
On the other hand, it does seem that the MHRA’s THR scheme works and you know what you are getting when you buy a herbal medicine. Otherwise charlatans and confidence tricksters would prevail.
These issues concern not only the campaign for medicinal cannabis but for cannabis law reform as a whole. Until we get to grips with them and develop a coherent approach we may find the UK continues to lag behind the rest of the world.
The Minister For Government Policy On The Strange Case Of Medicinal Cannabis.

Oliver Letwin MP
Oliver Letwin MP is, according to The Independent, “probably the most powerful person in the government after the Prime Minister and Chancellor”.
He is the Cabinet Office minister with responsibility for the implementation of government policy. He holds the ancient title of Chancellor of the Duchy of Lancaster. He is a member of 13 of the 14 Cabinet committees and chair of three of them, more than anyone other than Cameron. He is now chair of the most powerful of them, the Home Affairs committee, which Theresa May would have expected to chair and he also sits on nine of the 10 new “Implementation Taskforces”. Cameron is said to have told him “I need you with me every day”.
An extraordinarily powerful and influential man. I met with him last week to put the case for reform of policy on medicinal cannabis. He listened attentively, asked searching questions, evidently has a good understanding of science and medicines regulation. In the end, he agreed to ask Jeremy Hunt, Secretary of State for Health, to meet with me and a delegation of medicinal cannabis users. We agreed that the Home Office is no longer the route to reform. The word is that if the Department of Health calls for a new policy then the Home Office will comply. Theresa May has been sidelined on this issue. Her minister of state for drugs policy, Mike Penning, seems to be nothing but a mouthpiece for Home Office civil servants. Quite properly and at last, medicinal cannabis is being seen as a health issue and not one of law enforcement or criminal justice.
So we could not have a more important opportunity. Mr Letwin has now confirmed to me in writing that he will “..investigate the question of prescription cannabis for relief of medical conditions. I will start the process of talking to people in MHRA, Public Health England and so forth to try to get a sense of the pros and cons.”
Although he has not yet indicated to me that he supports our cause, he seemed particularly perplexed that cannabis is a schedule 1 drug whereas heroin is schedule 2 and may be prescribed by a doctor. It is clear that he recognises there is medicinal value in cannabis.
To have Oliver Letwin pursuing our cause through government is great progress. Although the loss of our Liberal Democrat allies has been a setback, it seems that the issue of medicinal cannabis has momentum. We need to keep on keeping on. Nothing works better than getting in front of government minsters and showing them that most people who use medicinal cannabis are responsible members of society, doing the best they can to contribute, holding down a job where possible, looking after their families and trying to maintain their health.
I sense that the optimism we felt before the election was not misplaced. Engaging with government, turning away from irresponsible protest and putting our arguments forward with courtesy and evidence is what will achieve our goal.
CLEAR Medicinal Users Panel. Fourth Delegation To Parliament.
 There is real momentum building in Parliament on the issue of medicinal cannabis. The first thing George Freeman said this week when he welcomed us to the Department of Health was: “There is a lot of discussion going on in government about this subject”.
There is real momentum building in Parliament on the issue of medicinal cannabis. The first thing George Freeman said this week when he welcomed us to the Department of Health was: “There is a lot of discussion going on in government about this subject”.
This is extraordinary progress, unimaginable as recently as 2012. Undoubtedly, developments in the US have raised cannabis up the political agenda. Through 2014, CLEAR has been well received by the Home Affairs Select Committee, the Home Office, the Department of Health, the Health Select Committee and just before Christmas I met with Baroness Meacher and Lord Howarth in the House of Lords. They are chair and treasurer, respectively, of the All Party Parliamentary Group for Drug Policy Reform. They are determined to push reform through to make medicinal cannabis available and have briefed one of the UK’s leading psychopharmacologists to prepare a review of existing evidence on the subject. Armed with this they have a plan to meet with key individuals in both Houses of Parliament and I have no doubt that they will succeed in changing minds.
Also this week, I met with advisors to Nick Clegg, the Deputy Prime Minister, in the very heart of government at the Cabinet Office. The Liberal Democrats are planning towards another coalition after the General Election and determined to see drugs policy form part of a new coalition agreement. Right at the front of their priorities is medicinal cannabis for which there is strong support from existing ministers, Lynne Featherstone at the Home Office and Norman Lamb at the Department of Health. Expect announcements in the run up to the election.
George Freeman is the Life Sciences Minister, responsible for medicines, NHS innovation, research, development, the MHRA and NICE. His role is as important as any other minister in achieving the reform we seek. He is another ally and has asked me to submit a paper setting out our proposals. Of particular importance is how medicinal cannabis could be regulated, either with a full Marketing Authorisation from the MHRA or possibly registration as a Tradional Herbal Medicine. The very fact that we are now discussing such detail is a measure of how far we have come.
So there is great cause for optimism at the start of 2015. We are closer than we have ever been before and this has been achieved by moving away from the old ‘protests’ and outdated campaigning ideas. I am confident that early in the new parliament we will see substantial progress.
Legal Opportunities For Medicinal Cannabis Users
Recent developments mean that there are new opportunities to challenge the prohibition of cannabis as medicine. Now I am not a lawyer, so these ideas should be carefully discussed with your legal advisors before you even consider pursuing any of them. I may be wrong about the correct procedure, process or terminology. I am highlighting opportunities that I have identified, based on my personal experience and knowledge. Qualified legal advice is essential.

Disingenuous
The British government’s current position on medicinal cannabis is absurd and irrational. As I understand it, those are exactly the criteria for which the process of judicial review is intended. That is one route. Another, more risky opportunity arises if you are facing prosecution or have been convicted of an offence of possession, cultivation or production. There are ideas here which you may want to consider as a defence or an appeal. However, please be very careful. If things go wrong, advancing such arguments might result in a heavier sentence, such is the cruel, oppressive and iniquitous intent of current government policy.

Dishonest
The Home Office is simply dishonest in its current stance saying that there “are no medicinal benefits” from cannabis. James Brokenshire, the drugs minister, cannot hide behind a lack of knowledge so he looks either more stupid or dishonest every day. David Cameron made the most dreadful, disingenuous comment about medicinal use in his Al Jazeera World View YouTube interview last week. See here. He said “That is a matter for the science and medical authorities to determine and they are free to make independent determinations about that.” That, of course, is absolute rot and Cameron should be ashamed of himself for such misinformation.
Obtain A Doctor’s Prescription For Medicinal Cannabis
There is nothing to prevent your British doctor from prescribing medicinal cannabis for you if he/she believes it is appropriate. Bedrocan BV is the official contractor to the Dutch government for the production of medicinal cannabis. Go to its website here and you will discover it has a range of products offering different proportions of cannabinoids and terpenoids for different conditions. Prescribing information is available for your doctor in exactly the same way as any other drug. All he/she has to do is select the product and write out a prescription in the normal way. Your doctor can’t get in trouble for this. There is nothing improper or unethical about it, but it is, of course, your doctor’s decision whether to do so or not.
 If your doctor isn’t prepared to help, the next best thing is to go to a doctor in Holland, Belgium, Germany, Spain or Italy, all countries where medicinal cannabis is regularly prescribed. In theory, you should be able to see a doctor in another EU country under reciprocal healthcare arrangements but if you can afford it, it may be simpler to go privately.
If your doctor isn’t prepared to help, the next best thing is to go to a doctor in Holland, Belgium, Germany, Spain or Italy, all countries where medicinal cannabis is regularly prescribed. In theory, you should be able to see a doctor in another EU country under reciprocal healthcare arrangements but if you can afford it, it may be simpler to go privately.
Another option is to go to one of the 15 US states that permit medical marijuana and obtain a doctor’s recommendation.
Once you have your prescription, you need to apply to the Home Office for a personal import licence to bring your medicine in from Holland. The licensing section on the Home Office website is here. If you obtain a licence you will also need to go through a similar process with the Dutch Bureau voor Medicinale Cannabis to obtain an export licence. The correct section of its website is here.
Of course, the reality is that the Home Office is not going to grant you a licence. You can then pursue the matter through your MP who should make representations to the minister on your behalf. You are then at the point to make an application for judical review of the Home Office’s decision.
Challenge The Government’s Interpretation Of The Schengen Agreement
The Schengen Agreement provides protection for travellers to carry their medicine with them within the EU. The crucial factor is your country of residence. See here for detailed information. Although there is no precise definition of residency, if you are resident in an EU country where medicinal cannabis is permitted, then you may bring your medicine into Britain and, believe it or not, there is no restriction on your use of it. You would be perfectly entitled to sit on the steps of Scotland Yard or even the Home Office’s Marsham Street HQ and smoke a spliff. However, if you are a UK resident, even if you have obtained your medicine on prescription abroad, you are not protected. This is clearly discriminatory under EU law and could be challenged in court. I’m not certain whether you would apply to a British court or to the European court but your solicitor would advise you on this.
Defence Or Appeal On The Grounds Of Medical Necessity
The Appeal Court disallowed a defence of medical necessity back in 2005. A petition to the House Of Lords Judicial Committee and to the European Court Of Human Rights was dismissed without any reasons given. I understand that the Appeal Court’s reasoning was that there were no proven medicinal benefits of cannabis. However, things have changed enormously since then. The MHRA approval of Sativex and the Home Office’s issue of a general licence for it are conclusive proof of medicinal value. Whatever misinformation the Home Office may promote, expert evidence would prove that Sativex is pharmacologically identical to, for instance, one of the Bedrocan products. There is also now a vast resource of peer-reviewed clinical evidence of medicinal benefits.
There is an horrendously improper judgement (R -v- David King, St Albans Crown Court), where a medicinal user was not allowed even to mention medicinal reasons to a jury on pain of imprisonment for contempt. Your lawyers would need to study this carefully. However, it is so clearly unjust that I do not believe it could be sustained.
 Re-Scheduling Of Sativex
Re-Scheduling Of Sativex
Sativex is currently a schedule 1 controlled drug which means it has no medicinal value. As mentioned earlier, the Home Office has dealt with this temporarily by issuing a general licence for it. However, it needs to be re-scheduled and the Advisory Council On the Misuse of Drugs (ACMD) has recommended that it be placed in schedule 4. See here for the full story.
Sativex cannot be re-scheduled under its brand name and the only pharmacologically accurate way of describing it is cannabis. The ACMD left a possible escape route for the Home Office by saying that its “active” ingredients would have to be specified. GW Pharma, the makers of Sativex would say that this means an extract of THC and CBD. However, this is dishonest. Sativex contains all the 60-odd cannabinoids that occur naturally in the plant. There is no other way of describing it accurately than to call it cannabis. If Brokenshire and his cronies try to prolong this deception then they can be challenged by judicial review. The aim here is to ensure that the re-scheduling is accurate and so cannabis becomes a schedule 4 drug. This would then open up all opportunities for cannabis as medicine.
I have no doubt now that medicinal cannabis will be permitted in some form or another in Britain within the near future. We may need to force the government’s hand through litigation or, perhaps Brokenshire will be moved to another department and then the Home Office can “adjust” its position.
At present, it is a monstrous injustice, an evil and obscene scandal, that those who need cannabis as medicine are denied it. The way of politics is that a few years from now it may well all have changed and Brokenshire will be at the Ministry of Silly Walks or somewhere better suited to his talents. However it works out, what I care about is that those in pain and suffering get the relief they need. One day soon, Brokenshire will have to answer to his constituents and later to an even higher power. How he will justify his cruelty and negilgence I don’t really care but I know I wouldn’t want to be in his shoes on judgement day.
Cannabis Embarrassment At The Home Office
 The re-scheduling of Sativex, the cannabis tincture marketed by GW Pharmaceuticals is causing huge embarrassment at the Home Office.
The re-scheduling of Sativex, the cannabis tincture marketed by GW Pharmaceuticals is causing huge embarrassment at the Home Office.
Everybody’s been able to go along with the white lie up to now that Sativex is some sort of highly complex, super scientific, super medicine containing cannabinoids. True enough, GW Pharma has put millions into development and testing in order to jump through the hoops the government has demanded. At the end of the day though, all Sativex consists of is a tincture, an alcohol extract of herbal cannabis. It’s made simply by gently heating a blend of herbal cannabis in ethanol and then adding a little peppermint oil to taste.

An Honourable Man?
The Medicines and Healthcare Products Regulatory Agency (MHRA) has approved Sativex for the treatment of muscle spasticity in MS. I understand that an approval for the treatment of cancer pain is expected shortly. The problem for the Home Office is that Sativex now has to be re-scheduled under the Misuse of Drugs Act 1971. Cannabis is presently in schedule one as having no medicinal value. The Advisory Council on the Misuse of Drugs (ACMD) has recommended this week that Sativex be in schedule four, alongside a variety of minor tranquilisers. However, as the ACMD says, “it will not be appropriate to refer to “Sativex”, which is a proprietary name, in any amendment to the misuse of drugs regulations, and that a suitable description of the relevant component(s) of “Sativex” will have to be scheduled.”
This is going to be tough for James Brokenshire to face up to. GW specifies that Sativex contains approximately equal proportions of THC and CBD but that’s not the whole truth. It also contains as many as 400 other chemical compounds which occur naturally in the plant including at least 85 cannabinoids (nobody is exactly sure how many cannabinoids there are or their effects). You see there’s not really any other accurate way of describing Sativex except to call it cannabis. So how can Mr Brokenshire possibly move it to schedule four? He endlessly repeats the propaganda that “there are no medicinal benefits in cannabis”.
Either Mr Brokenshire has to come clean and accept that his past position was incorrect or he has to promote some further deception.
I trust he will prove to be an honourable man.
Advisory Council On The Misuse of Drugs Meeting, 18th November 2010
I attended this meeting last Thursday at Church House, just around the corner from the Houses of Parliament.
There were approximately 35 members of the council in attendance, sitting around a huge U shaped table with perhaps 20 people in the public seats. Inevitably, such a huge meeting could only touch on adminstrative matters and formalities. Clearly, most of the ACMD’s work is done in much smaller working groups. However, there was an interesting Q&A session and I was pleased to experience a council meeting. I wouldn’t recommend it for light entertainment though!

Prof. Leslie Iversen
Professor Leslie Iversen was in the chair for the last time. His post and those of eight other members have been advertised and their replacements will be appointed as from 1st January 2011. These are voluntary positions with members receiving only expenses and subsistence payments for their work. They undertake an onerous and important responsibility and I commend them for their public service.
Full minutes should be available on the Home Office website here within a few weeks. However the main items of interest were:
- the ACMD’s response to the Home Office’s drug strategy consultation
- a report on anabolic steroids
- a report on the issuing of foil by drug clinics as an alternative to injection
- a report on 2-DPMP, marketed as the “Ivory Wave ” legal high
- a request to report on khat, the herbal product from East Africa that contains cathinone, the same active ingredient as mephedrone
- a request to report on cocaine use after a recent report placed Britain at the top of the European league table
Then we came to the Q&A session and, of course, yours truly had a question prepared. First though there was a large contingent of the Somalian community present appealing for the prohibition of khat.
I have to say that nothing I have heard about either mephedrone or khat has interested me or persuaded me to experiment. There were a number of emotional and passionate speeches rather than questions; one from an ex-khat addict, one from a Somalian psychiatrist and others from community members. It’s clear that khat does cause harm but it saddened me that the only solution being suggested was prohibition. I understand this as a knee jerk reaction but it won’t work. All it will do is drive use undergroud and make the problem worse. Professor Iversen himself commented that the price of khat where it has been banned is 20 times that of where it is legal. If prohibition is enacted in Britain all we will be doing is playing straight into the hands of criminal gangs yet again.
I asked the council whether there wasn’t an urgent need for it to update its advice to the government on the medicinal benefits of cannabis. I cited the recent MHRA approval of Sativex which is, of course, nothing more than a tincture of herbal cannabis. I also mentioned that Arizona had just become the 15th state in America to introduce a medical marijuana programme and that Israel has recently announced a massive increase in growing facilities and dispensaries.
I am paraphrasing here, of course, but Professor Iversen threw up his hands in horror at being asked to review cannabis again when he has already done so three times. The general view from the council seemed to be that whatever was said to government on this subject, no notice would be taken. I shall be following up my oral question with a letter to Profesor Iversen. We have to expose this Home Office lie that there are no medicinal benefits from herbal cannabis and that this is based on advice from the ACMD. It isn’t. It’s a government deception.
For me the most important part of the day was the opportunity to introduce myself in person to Professor Iversen. I thanked him for agreeing to become a founder council member of the British Medicinal Cannabis Register. He said how enthusiastic he was about the register and that he has been an advocate of medicinal cannabis since the 1990s.

